Congress May Kick the Can Again on the Doc Fix
Repeating a story heard many times before, in a speech at a Federation of American Hospitals conference, House Ways And Means Chairman Paul Ryan (R-WI) indicated (subscription required) that a permanent replacement for the Sustainable Growth Rate (SGR) formula was not likely to pass by the March 31 deadline, and instead that lawmakers would do a short-term "doc fix" to buy more time.
The expiration of the current doc fix, one of this year's Fiscal Speed Bumps, would cause a 21 percent cut in Medicare physician payments starting in April as dictated by the SGR. That lawmakers are doing a short-term doc fix is unsurprising -- it's been standard operating procedure since 2003 -- but it is disappointing because they are as close to enacting a permanent replacement as ever before. Congress just isn't willing or able to agree on offsets to pay for it at this time.
What makes this situation different than previous times where lawmakers had to deal with the doc fix is that there is a bipartisan and bicameral agreement on a replacement system that would promote alternative physician payment models, and help transition away from fee-for-service payment. But while coming up with the replacement may no longer be an obstacle, the $175 billion cost through 2025 (up from $140 billion previously) apparently is, despite the fact that there are countless health care savings options available.
Our PREP Plan came up with $170 billion of savings through 2024 (adding in 2025 would bring this easily above $175 billion) through a combination of improving provider and beneficiary incentives. The appendix of that report also provides several other options that can produce tens of billions more in savings. The fact that lawmakers may have to resort to another short-term patch shows the downside of waiting until the last minute to fix a problem: they will need to spend time to negotiate a package, thus waiting takes that option off the table.
Policies in the PREP Plan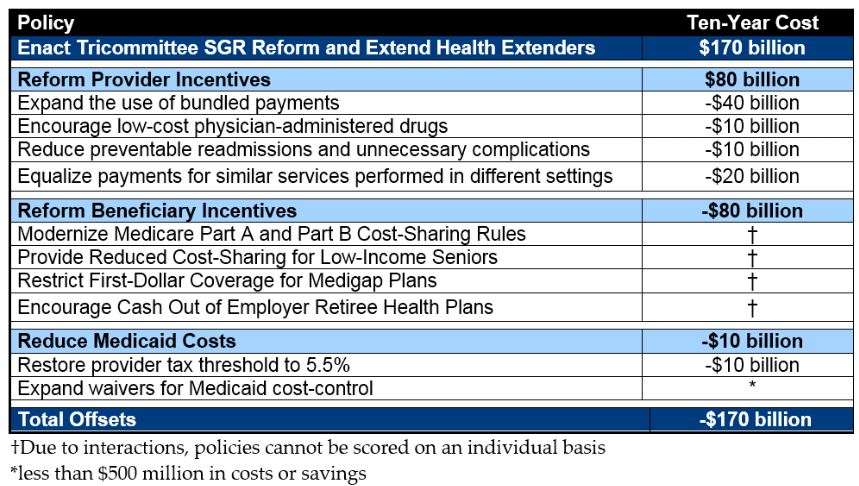
If lawmakers are to resort to another short-term fix, though, they should continue with the precedent of offsetting its cost. According to CBO, a nine-month freeze through the end of 2015 would cost $12 billion, and a 21-month freeze through the end of 2016 would cost $30 billion (obviously, a shorter-term patch would cost less).
Judging by past experience, one likely way to offset this cost would be to extend the sequester on mandatory spending and the ACA's Medicaid Disproportionate Share Hospital cuts by one year to 2025, saving nearly $15 billion. These would also, however, be among the least productive ways because they would offset first and second year costs with tenth year savings that are not new and temporary -- but they would still satisfy pay-as-you-go rules. A much better alternative would be to use permanent savings from new policies that can help bend the health care cost curve. Below are examples of such policies.
| Possible Short-Term Doc Fix Offsets | |
| Policy | Savings Through 2025 |
| Encourage use of generic drugs by low-income beneficiaries | $25 billion |
| Increase Medicare Advantage coding intensity adjustments | $15 billion |
| Expand readmission and avoidable complication penalties | $10 billion |
| Encourage low-cost physician-administered drugs | $10 billion |
| Reduce subsidies for medical education | $10 billion |
| Bundle payments for post-acute care | $10 billion |
| Extend mandatory sequester by one year to 2025 | $10 billion |
| Increase the Medicaid drug rebate | $8 billion |
| Prohibit manufacturers from making agreements to delay generic drugs | $4 billion |
| Extend Medicaid DSH cuts by one year to 2025 | $4 billion |
Source: CBO, OMB
If/once they pass a short-term fix, they should get to work right away developing offsets for the SGR replacement. Buying time is only useful if lawmakers use that time wisely.


