CBO Finds House VA Bill Could Cost More, Does Cost Less Than Senate Bill
The Congressional Budget Office today released a preliminary analysis of several sections of the House VA reform bill. Like the Senate bill that we analyzed last week, the legislation would increase VA health spending by allowing the VA to contract with private health providers. In fact, if appropriators fully funded the House legislation, it could cost more than the Senate bill. Unlike the Senate bill, the legislation would not create a significant mandatory appropriation and therefore would not add significantly to the deficit without further action from Congress.
As the House and Senate prepare to go to conference on the VA bills, we hope they find ways to efficiently target expanded benefits, and we especially hope they propose paying for any new costs. More importantly, we believe the conference committee should ensure new funding levels are set either by the appropriators, by the legislation itself (through a capped mandatory appropriation), or preferably by both (a fixed discretionary authorization); not by offering the VA a blank check.
When it comes to proposed changes to the VA health system, the House and Senate bills are quite similar. Specifically, both would allow and require the VA to contract with private health care providers to help reduce the VA backlog.
There are also a number of differences. Among those identified by CBO, the House bill would require the VA to target a two-week waiting period (CBO estimates the VA would target one month under the Senate bill), and the House bill would allow the VA to reimburse certain noncontracted health care.
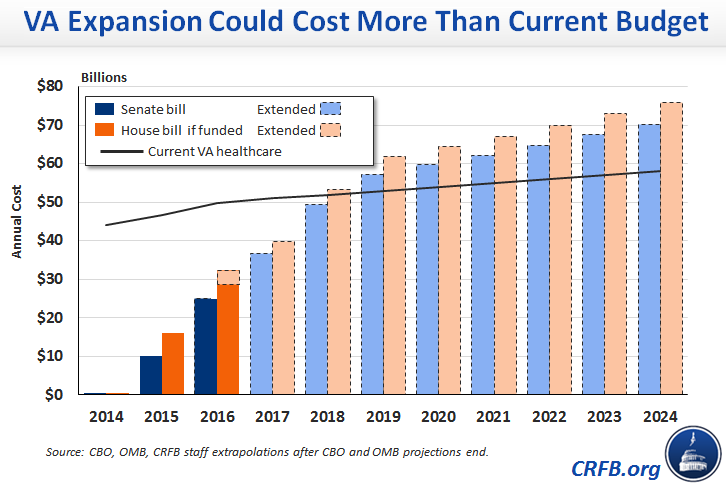
As a result of these changes, the House bill would have the potential to cost more than the Senate bill if fully phased in – about $54 billion as opposed to $50 billion per year. In addition, it would phase in somewhat faster – CBO estimates it would be about 60 percent phased in by 2016, compared to 50 percent for the Senate bill.
| Senate Bill (Title III) | House Bill (Sections 2 & 3) | |
| The Legislation | ||
| How is funding provided? | Open-ended mandatory funding | Subject to discretionary appropriations |
| Who decides additional spending levels? | The Department of Veterans Affairs | The appropriations committees |
| How long is the target "wait-time"? | VA's discretion (CBO assumes 30 days) | 14 days |
| How can the VA pay providers? | On a contract basis | On a contract or ad hoc basis off of Medicare or Tricare rates |
| When does the expansion end? | September 30, 2016 | July 31, 2016 |
| The CBO Score | ||
| What is the potential cost if fully phased in? | $50 billion per year | $54 billion per year |
| What is the total cost of the legislation if funds are fully appropriated? | $35 billion over 10 years | $44 billion over 10 years |
| How much does the legislation itself increase deficits? | $35 billion over 10 years | ~$1 billion over 10 years |
| Additional Analysis | ||
| How much would the bill cost if fully funded and extended for ten years? | ~$500 billion | ~$550 billion |
As a result of these differences, CBO estimates the House plan could cost $44 billion in total, compared to $35 billion for the Senate plan.
But importantly, the vast majority of that spending is contingent on future appropriations – which under current law are bound by discretionary spending caps. Sections 2 and 3 of the legislation would increase deficits by less than $1 billion by allowing the VA to fund a small portion of the new program immediately with unobligated funds that would not otherwise be spent.
Rather than providing the authority to increase spending directly, as in the Senate bill, the House bill requires the Office of Management and Budget to provide an estimate of the potential costs and request additional budget resources as necessary. Without violating the caps or providing an emergency designation, appropriators would have to reduce spending elsewhere to make room for new VA spending. To the extent they could not identify enough savings, they could scale back the funds provided to the VA to contract with private providers.
Still, a desire to fully fund this legislation could create pressure for a supplemental spending request which uses an emergency designation to circumvent discretionary caps. Once in place, there could also be pressure to continue this benefit beyond 2016.
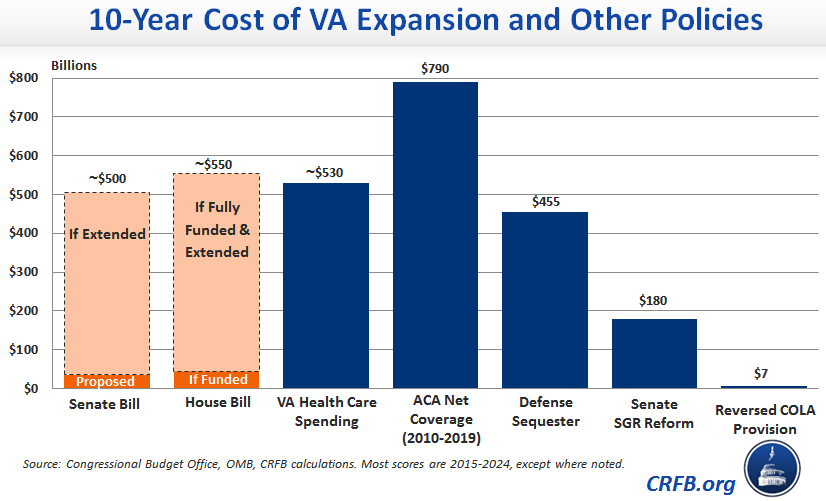
Given that, it is worth understanding the potential implications of expanding the VA’s authority if Congress chooses to fully fund and continue this bill. We estimated last week, very roughly, that Title III of the Senate legislation could cost about $500 billion over ten years if continued on a permanent basis. Similarly, Sections 2 and 3 of the House bill, if appropriated in full and continued on a permanent basis, could cost more than $550 billion over ten years.
If the expansion did end up costing $550 billion over the next decade, that would be more than the entire expected cost of the current VA health care spending, significantly more than the cost of repealing the defense sequester, and about three times as much as the permanent SGR reform bill Congress refused to offset, and therefore could not pass, earlier this year.
To be sure, the problems at the VA are real and our nation’s veterans have real unmet needs that Congress must address. But budgeting is about prioritizing.
Within the legislation itself, that means Congress must decide what is a reasonable waiting period, how much they are willing to pay provide providers, whether they want to offer this benefit to veterans not currently enrolled in VA health care (which would represent about two-fifths the cost of the House bill and could create additional pressure on the VA after the program ended), and whether they can better target this benefit to those veterans truly in need. It also means identifying what lower priority spending or tax breaks can be reduced, repealed, or reformed in order to make space for this benefit. Last week, CRFB listed a large number of potential offsets.
To ensure this prioritization is happening, the conference Committee should leave these decisions in the hands of the appropriators, or else provide the VA a fixed amount of funds which is fully paid for with changes elsewhere in the budget.

